17: Odds Ratios from Case-Control Studies version:
9/23/06
Review Questions
- How do case-control studies differ from cohort
studies?
- Why are case-control studies unable to estimate incidence or prevalence?
- What symbol is used to denote the odds ratio parameter? What symbol is used
to denote the odds ratio estimator?
- Before calculating a confidence interval for the odds ratio, we converts
the odds ratio
estimate to a ______________ scale.
- List the null hypothesis tested by case-control data.
- When is Fisher's test used in place of a chi-square test?
- In a 2-by-2 table for matched-pair data, table cells t and w contain counts
for ____________ pairs,
while cells u and v contain counts for ___________ pairs.
- True or false? In matched case-control studies, information about concordant pairs is ignored.
- What is the name of the chi-square statistic used to test matched-pair data?
- What is the primary benefit of matching?
- [T or F?] You can use a 95% confidence for the odds ratio to determine
statistical significance at alpha = 0.05.
- [T or F?] You can use a 95% confidence for the odds ratio to determine
statistical significance at alpha = 0.01.
- How do you use a 95% confidence for the odds ratio to determine statistical
significance at alpha = 0.05?
- Which of the following 95% confidence interval for odds ratios are
significant at alpha = 0.05? (a) 0.01 to 0.77 (b) 0.77 to 1.23 (c) 1.23 to 2.43
Exercises
Part A: Independent Samples
17A.1
Wynder
and Graham's
case-control
study of smoking
and lung cancer. A
historically important study published compared
the smoking histories of 605 cases with lung cancer to 780 controls
without cancer. Data on average use of tobacco during the past 20 years was classified as
follows:
-
5 = Chain smoker (35 cigarettes of more per day for at
least 20 years)
-
4 = Excessive smoker (21 � 34 cigarettes per day for
more than 20 years)
-
3 = Heavy smoker (16 � 20 cigarettes per day for more
than 20 years)
-
2 = Moderately heavy smoker (10 � 15 cigarettes per
day for more than 20 years)
-
1 = Light smoker (1 � 9 cigarettes per day for more
than 20 years)
-
0 = Non-smoker (less than 1 cigarette per day for more
than 20 years)
If the patient smoked for less than 20 years, the amount of smoking was
reduced in proportion to its duration.
Cross-tabulation revealed (Wynder
& Graham, JAMA,
1950. click names for biographies; click citation for article reprint):
|
Smoking
|
Cases
|
Non-cases
|
|
5
|
123
|
64
|
|
4
|
186
|
98
|
|
3
|
213
|
274
|
|
2
|
61
|
147
|
|
1
|
14
|
82
|
|
0
|
8
|
115
|
|
Total
|
605
|
780
|
Calculate odds ratio for each level of smoking using the non-smokers as the
reference group. (Optional: Determine 95% confidence
intervals for each estimate.) Interpret these results.
17A.2 Cell phone use and brain tumors. Results
from two case-control studies on cell phone use and brain cancer are
summarized below. Review each summary and discuss whether the study in question
supports or does not support the theory that recent
use of hand-held cellular telephones causes brain tumors. Explain your
reasoning in each instance.
(A) A case-control study by Inskip
and co-workers (2001) examined the
use of cellular telephones between 1994 and 1998 in 782 cases with various forms
on intracranial tumors and 799 controls admitted to the same hospitals for a
variety of nonmalignant conditions. Subjects were considered exposed if
they reported use of a cellular telephone for more than 100 hours. The odds
ratio (OR) for glioma was 0.9 (95 percent
confidence interval 0.5 to 1.6), the OR for meningioma was 0.7 (95 percent confidence
interval 0.3 to 1.7), the OR for acoustic neuroma 1.4 (95 percent confidence interval 0.6
to 3.5), and the OR for all tumor types combined: 1.0 (95 percent confidence interval 0.6
to 1.5)
(B) A case-control study by Muskat
and co-worker (2000)[full text] conducted between 1994 and 1998 used a structured questionnaire to
quantify the statistical relation
between cell phone use and primary brain cancer in 469 cases and 422 matched controls.
The results of the study stated "The median monthly hours of use were [sic]
2.5 for cases and 2.2 for controls. Compared with patients who never used
handheld cellular telephones, the multivariate odds ratio (OR) associated with
regular past or current use was 0.85 (95% confidence interval [CI], 0.6-1.2).
The OR for infrequent users (<0. 72 h/mo) was 1.0 (95% CI, 0.5-2.0) and for
frequent users (>10.1 h/mo) was 0.7 (95% CI, 0.3-1.4). The mean duration of
use was 2.8 years for cases and 2.7 years for controls . .. The OR was
less than 1.0 for all histologic categories of brain cancer except for uncommon
neuroepitheliomatous cancers (OR, 2.1; 95% CI, 0.9-4.7)."
17A.3 Esophageal cancer and tobacco consumption
(dichotomized exposure).
This exercise considers tobacco
use with exposure dichotomized at 20 gms/day on the risk of esophageal cancer in
the bd1.sav data set (right-click data set
name to download file).
Data are originally
from Tuyns
and coworkers (1977) as reported by Breslow and Day
(1980). Cross-tabulation reveals:
|
Tobacco
|
Cases
|
Non-cases
|
|
20+ g/day
|
64
|
150
|
|
0-19 g/day
|
136
|
625
|
(A) Calculate the odds ratio and its 95% confidence interval.
Interpret your result.
(B) Using a chi-square statistic, derive a P-value for the problem.
(C) Download bd1.sav
(right-click > Save as). After
downloading the file, open it in SPSS and print the code book by clicking File > Display Data Info
> bd1.sav > OK. Keep the codebook handy for future reference.
(D) Cross-tabulate the data
by clicking Analyze > Descriptive Statistics >
CrossTabs. Select TOB2 as the row (exposure) variable and CASE
as the column (outcome) variable. Click the statistics button and check the
boxes for Chi-square
and Risk . Click Continue > OK. Do the
results in SPSS confirm your earlier calculations?
17A.4 The Oxford Childhood Cancer Survey. The file bd2.sav contains data from a case-control study
on childhood
leukemia and in utero X-ray exposure (Breslow & Day, 1980, p. p.
240). Cases are children less than 10 years of
age with leukemia or lymphoma occurring in the period 1954-65. Controls are similarly aged children from the same neighborhood.
Data are stored in the variable CASE: (1 = case, 2 = control). In utero exposure to diagnostic
radiography is stored in the variable XRAY: (1 =
yes, 2 = no). [Original data are matched-pairs. We have ignored the match. In
practice, ignoring the match is not
recommended but this instance, makes little difference in risk estimates.]
(A) Download the dataset bd2.sav
and then cross-tabulate the data. Show data as a 2-by-2 table XRAY
as the row variable and CASE as the column variable.
(B) Calculate the odds ratio and its 95% confidence interval.
Interpret your findings. Do data support
the hypothesis that in utero X-ray exposure increases the likelihood of childhood
leukemia & lymphoma?
(C) Perform a chi-square test of H0:y = 1.
17A.5 Doll & Hills, 1950. A historically
important case-control study of smoking and carcinoma of the lung was completed
by Doll & Hill
in 1950. They found 647 of the 649 lung cancer cases
were smokers compared with 622 of 649 controls. (Click here
for a reprint of the original article.) Display thee data in 2-by-2 crosstab and calculate
the odds ratio. Include a 95% confidence interval for
the odds ratio parameter, and interpret your results
17A.6 IUDs and infertility.
A case-control study of contraceptive devices and
infertility found prior use of intra-uterine devices (IUDs) in 89 of 283 infertile
cases. In contrast, 640 of 3833
fertile control women had used IUDs (Cramer et al.,
1985; Rosner, 1990, p. 381). Data are shown in a 2-by-2 table, below. Calculate the odds
ratio and its 95% confidence interval. Interpret the results.
|
IUD
|
Cases
|
Non-cases
|
|
+
|
89
|
640
|
|
-
|
194
|
3193
|
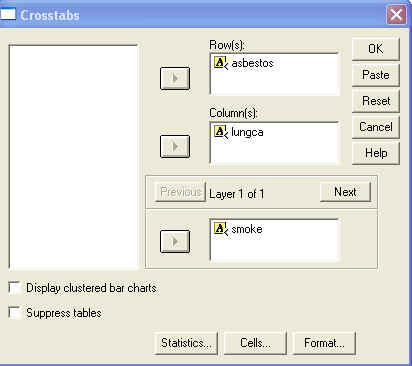
17A.7 Asbestos, cigarettes, and lung cancer. Data
stored in asbestos.sav are from a case-control study on lung cancer, asbestos exposure, and
smoking. Right-click the file name to download the dataset. By going through the steps listed below, you will
learn about interaction.
(A) Cross-tabulate LUNGCA (column variable) by SMOKE (row
variable). Determine the odds ratio.
(B) Cross-tabulate LUNGCA by ASBESTOS. Determine the odds ratio.
(C) Cross-tabulate LUNGCA by ASBESTOS stratified by by SMOKE. This
is accomplished
by filling in the SPSS dialogue box shown below. Calculate odds ratios
separately for smokers and non-smokers. Are these odds
ratios homogeneous or heterogeneous?
17A.8 Esophageal cancer and alcohol recorded at
four levels. This data set
was introduced in StatPrimer. In StatPrimer, alcohol consumption was
dichotomized at 80 g/day. However, data were initially recorded at four different levels of alcohol
consumption (0-39, 40-79, 80-119, 120+). You can calculate the odds ratio
associated with these increasing levels of exposure by comparing each exposure level to the
baseline provided by the least exposed group. Calculate the odds ratio for each
table below and interpret the results. Is there evidence of a dose-response
relationship?
Low vs. very low alcohol consumption
gms/day Cases Controls
40-79 75 280
0-39 29 386
Intermediate vs. very low alcohol consumption
gms/day Cases Controls
80-119 51 87
0-39 29 386
High vs. very low alcohol consumption
gms/day Cases Controls
120+ 45 22
0-39 29 386
17A.9 Vasectomy and prostate
cancer. Data from a case-control study on vasectomy and prostate
cancer are cross-tabulated below (Zhu et al.,
1996). Calculate the odds ratio and its 95% confidence interval. (Optional: Calculate the P-value for the
problem.)
17A.10 Brain tumors and electric blanket
use. A case-control study assessed the risks of brain tumors associated
with
electric blanket use. Cross-tabulated data are shown below and are also stored
as individual records in BRAINTUM.SAV
(Preston-Martin et al.,
1996). Calculate the odds ratio and its 95%
confidence interval. Discuss the results.
|
|
Cases
|
Non-cases
|
|
El.
blanket +
|
53
|
102
|
|
El.
blanket -
|
485
|
693
|
17A.11 Baldness and the risk of heart attack. Both baldness and heart attacks are more common in males
than in females. Is there a link between the two? The answer to this question
takes on importance when treatments for baldness are considered. Minoxidyl, a
treatment for baldness, is effective in some cases of male pattern baldness when
applied topically. If the underlying condition of baldness elevates the risk of
cardiovascular diseases, then any increase in the risk of cardiovascular disease
in Minoxidyl users might mistakenly be attributed to the drug and not to the
underlying condition of baldness. A study by Lesko
and co-workers (1993) addressed this question by looking at data for 722 controls and 665
heart attack cases.
Subjects were
under 55 years of age who were admitted to hospitals in Massachusetts and Rhode Island.
(Staff from the School of Public Health at the Boston University School of
Medicine telephoned the hospitals to locate eligible cases.) Cases were men
admitted for and survived a first heart attack with no prior serious heart
problems. Controls were men admitted to the hospitals for non-fatal, non-cardiac
problems. Control subjects with a prior history of heart disease were excluded from the study.
Cases and controls were interviewed, and the degree of male pattern baldness was determined on a
scale of 1 (no baldness) to 5 (extreme baldness). Data are cross-tabulated
below:
(A) Describe the association
between baldness and heart attacks by either calculating exposure proportions in
cases and controls or by calculating odds ratios associated with each level of
baldness using baldness
category 1 as the reference category.
(B) Conduct a chi-square test for overall association
(C) Optional: Perform a test for trend.
(D) Consider lurking variables that might explain the
observed association, i.e., consider potential confounders.
|
Baldness
|
Cases*
|
Controls
|
|
1 (none)
|
251
|
331
|
|
2
|
165
|
221
|
|
3
|
195
|
185
|
|
4
|
50
|
34
|
|
5
(extreme)
|
2
|
1
|
|
Total
|
663
|
772
|
Part B: Matched-pairs
17B.1 Fruits, vegetables, and adenomatous
polyps. A case-control study by Witte
and co-workers (1996) used
matched-pairs to
study the risk
of adenomatous polyps of the colon in relation to diet. All cases and controls had undergone sigmoidoscopic
screening. Controls were matched to cases on time of screening, clinic, age, and sex.
One of the study's analyses considered the effects of
low fruit and vegetable consumption on colon polyp risk. There were 45 pairs in
which the case but not the control reported low fruit/veggie consumption. There were 24 pairs in which the control but not the case reported
low fruit/veggie consumption [Summary counts reported in Rothman & Greenland, 1998,
p. 287;
same data used in StatPrimer as an illustrative
example.]
(A) Calculate the odds ratio associated with low fruit/veggie consumption. Interpret
this result.
(B) Calculate a 95% confidence interval for
the odds ratio.
(C) Use a continuity-corrected
McNemar statistic to calculate a P-value for the data.
(D) Do data support the proposed connection between low fruit/veggie
consumption and colon cancer?
17B.2 Smoking
and mortality in identical twins. When smoking was first suspected
as a cause of disease, Sir Ronald Fisher offered the constitution
hypothesis as an explanation for the observed association. Fisher (1957,
1958a,
1958b)
did not entirely dispose of the causal hypothesis, however.) The constitutional
hypothesis suggested
that people genetically disposed to lung cancer were more likely to smoke.
In other words, the relation between smoking and disease was confounded by
constitutional factors. The constitutional hypothesis was put to the ultimate test by a study in which 22
smoking-discordant monozygotic twins where studied to see which twin
first succumbed to death (Kaprio & Koskenvuo,
1989). In this study, the
smoking-twin died first in 17 of the pairs (i.e., u = 17, while
u + v = 22). Calculate the odds
ratio for these data. Calculate a P-value
for testing H0:  =
1. Interpret your findings. Which theory is refuted? Which is supported? [Same as StatPrimer illustrative
example.]
=
1. Interpret your findings. Which theory is refuted? Which is supported? [Same as StatPrimer illustrative
example.]
17B.3 Collaborative Group Study of Stroke in Young Women,
hemorrhagic stoke. The
Collaborative Group
Study of Stroke in Young Women
(1975) was a
case-control study of cerebrovascular disease
and oral contraceptive use in women between 14- to 44-years of age completed in
the 1970s. Cases were matched
to neighborhood
controls according to the age, sex, and race.
(A) Here are the matched data for thrombotic stroke (Lilienfeld & Lilienfeld,
1980, p. 220).
Calculate the odds ratio for these data.
|
Matched-pairs
|
Control exposed
|
Control
non-exposed
|
Total
|
|
Case
exposed
|
2
|
44
|
46
|
|
Case
non-exposed
|
5
|
55
|
60
|
|
Total
|
7
|
99
|
106
|
(B) Suppose the match was broken and the investigators had analyzed the
data unaware of the importance of matched-pair analyses. Rearrange the data in
the above table to portray how it would look in an unmatched 2-by-2
cross-tabulation showing the number of exposed cases, exposed controls and so on. Then,
calculate the odds ratio for these unmatched data. How does this compare to the
results achieved with the proper matched analysis.
17B.4 Collaborative Group Study of Stroke in Young Women,
hemorrhagic stoke. Exercise 17B.3 introduced thrombotic
stroke data from the Collaborative Group Study of Stroke
in Young Women. The hemorrhagic stroke data are shown below. Analyze the data in matched and unmatched
format, as you did in exercise 17B.3. Compare the two analyses.
|
Matched-pairs
|
Control exposed
|
Control
non-exposed
|
Total
|
|
Case
exposed
|
5 |
30 |
35 |
|
Case
non-exposed
|
13 |
107 |
120 |
|
Total
|
18 |
137 |
155 |
17B.5 Estrogen and cervical cancer. Data from a matched case-control study of conjugated
estrogen use and cervical cancer by Antunes
and co-workers (1979) are shown below (Abramson & Gahlinger, 2001, p.
137). Calculate the odds ratio and its 95% confidence interval. In
addition, calculate a P-value for the problem. Interpret your results.
|
Matched-pairs
|
Control exposed
|
Control
not exposed
|
Total
|
|
Case
exposed
|
12 |
43 |
55 |
|
Case not
exposed
|
7 |
121 |
128 |
|
Total
|
19 |
164 |
183 |
Key to Odd Numbered Problems
Key to Even Numbered Problems (may not be posted)